In this issue
- Celebrating arthritis research (2000-2015)
- “Treat-to-target” and “window of opportunity”: what do they mean for you?
- How do Canadian arthritis researchers stack up against the world?
- Putting research to work: Public, private, patient program receives CIHR Partnership Award for arthritis screening program
- ACE Participation at CRA Annual Conference
JointHealth™ insight Published February 2015

Turn back the clock 15 years ago when Arthritis Consumer Experts was founded, when new research began to suggest that osteoarthritis started attacking joints long before middle age, even before a person experienced symptoms of pain and inflammation. A paradigm shift in arthritis understanding was occurring and would deeply impact patients and their families, government and employers. Back in 2000, the world for people with arthritis was on the verge of dramatic transformation based on this new research and with the introduction of biologic therapy for inflammatory types of arthritis, like rheumatoid arthritis, a driver of indirect healthcare costs and a leading cause of work disability in Canada. Fast-forward to today and the scene looks much different. With well-trained Canadian researchers continuing to work and lead in collaboration with their counterparts around the world, the words “prevention” and “remission” are heard in rheumatology offices across the country. Pain is being reduced, quality of life is improving, and work disability is dropping in people with arthritis who would have done much worse had the knowledge from research not been utilized in their model of care.
In this JointHealth™ monthly, we look at research stories that demonstrate the value of collaboration between those who conduct research and those who use its results – consumers like us, people living with arthritis.
This collection of stories highlights the significant impacts arthritis research can achieve. Although each is different, as a group, they exemplify the commitment of Canadian researchers to improving the health of Canadians living with arthritis.
“Treat-to-target” and “window of opportunity”: what do they mean for you?

Opening a “window of opportunity”
With no arthritis cure available, doctors in the past did little more than manage a patient’s pain, explains Dr. Kam Shojania, a rheumatologist and Clinical Professor and Chief, Division of Rheumatology, The University of British Columbia.
“Now, we see that the best therapy is early,” he says, adding that if doctors prescribe disease-modifying drugs for inflammatory forms of arthritis within the early weeks or first six months of disease onset, the chance of putting them into long-term remission go up significantly.
“If you miss that window of opportunity, it’s very sad. You can still treat it, but you are not going to put them in remission. And any damage that has already occurred prior to proper treatment can never be reversed.”
The “window of opportunity” for early treatment of rheumatoid arthritis (RA) within six weeks after positive diagnosis is critical to help avoid or lessen joint damage, produce disease remission and preserve joint integrity since it is documented that joint damage begins within this time frame. For example, if a person with newly diagnosed RA is started on triple DMARD therapy, the need for stronger, more expensive medications will be delayed or not needed all together. As well, biologic response modifiers have exhibited significant clinical benefit in the treatment of early RA (methotrexate naïve patients) and also when used together with methotrexate.
The "treat-to-target" concept
Another treatment paradigm for arthritis involves physicians adopting an approach that all RA should be put into remission (remission as the treatment target), with patients nearly, or completely, free of inflammation, pain and other hallmark symptoms. Central to this treatment philosophy is aggressively initiating and swapping medications every two or three months until the therapy combination brings the disease under maximal control.
This concept is called “treat to target” and historically has been used to help with chronic medical conditions like diabetes, high blood pressure, and high cholesterol. The majority of rheumatologists in Canada, the United States and Europe are now taking this approach with their RA and other inflammatory arthritis patients.
Previously, rheumatologists took a more cautious approach to improve symptoms in their patients, which led to smaller improvements of overall health over a longer period of time, measured by percentages (20% or 50%, for example). Today, they work closely with their patients and set a decisive treatment goal – to achieve 100% improvement. Following the “treat-to-target” concept, complete disease control is the focus and means that if successful, patients get their lives back, avoid the permanent joint damage and many of the other negative consequences that RA can cause over time.
The latest research is focused on developing “prediction tools” for the purpose of matching the right quantity and level of care to the right person. This requires following people with newly diagnosed onset RA closely. Central to “treat to target” is rheumatologist and patient assessing all treatment options available, considering which treatment, alone or in combination, is best and setting improvement goals, measuring progress towards them, and then adjusting or continuing with the treatment until complete remission is achieved if at all possible.
Measurements for gauging success can include:

Canada has a strong track record as an international leader in arthritis research. At the recent American College of Rheumatology Annual Meeting (November 2014), attended by leading researchers from around the world, studies led by Canadians were plentiful. Here are some of the notable findings presented:
Tools to help arthritis patients self monitor their disease
Erin Carruthers, a Research Assistant at Arthritis Research Canada, led a presentation on “Using patient reported outcome measures to classify disease activity states in rheumatoid arthritis: A Comparison of Patient Activity Score (PAS) and Routine Assessment of Patient Index Data (RAPID)”.
Helping people with rheumatoid arthritis monitor their own disease activity enhances active involvement of people in their care and may help the “treat to target” strategy by alerting patients when targets are not met, indicating a need to see their physician and re-evaluate treatment. The study compared patient reported outcomes to evaluate disease activity by measuring their agreement with disease activity states evaluated by their rheumatologist at the time of a follow-up visit. The results suggest that patients can self-monitor their disease activity using the self-reported questionnaires. One questionnaire, PASII, showed the best agreement with rheumatologist assessments.
Medications in pregnancy for lupus patients
Dr. Mary De Vera, Assistant Professor at UBC’s Faculty of Pharmaceutical Sciences, and her team reported on their study on “Patterns of medication use before, during, and after pregnancy among women with systemic lupus erythematosus: A population-based study”.
Dr. De Vera’s team assessed the use of medications in pregnant women with lupus in British Columbia. Most pregnancy trimesters in the study were exposed to hydroxychloroquine and/or chloroquine (41 to 45% of exposed pregnancy trimesters). The research observed an increase in glucocorticosteroid (like prednisone) exposures during pregnancy, as well as post-delivery. Findings emphasize the importance of counseling women regarding childbearing decisions as well as the need for evaluation of the risk-benefit profiles of medications in pregnancy.
Arthritis and a First Nations population
Dr. Cheryl Barnabe, a leading researcher at the University of Calgary, has lead a team of researchers on a study on the prevalence of inflammatory arthritis diseases in the First Nations population of Alberta.
Rheumatoid arthritis, ankylosing spondylitis and reactive arthritis were estimated as being twice as frequent in the First Nations population. This research study found, in contrast, psoriatic arthritis was slightly less frequent in First Nations. Crystal arthritis like gout surpassed rheumatoid arthritis as the most frequent type of inflammatory arthritis in the non-First Nations population, with a frequency three times that of the First Nations cohort.
Patients and healthcare professionals using technology
Dr. Anne Townsend, Research Associate, Department of Occupational Science and Occupational Therapy at the University of British Columbia, shared findings from her team’s research on “Aligning ethics with digital health technologies and shared decision-making: Interview accounts of patients and clinicians”.
Patients with different types of arthritis and at least one other health condition, and healthcare providers were interviewed to find out how they used different types of new health technologies such as the Internet for online information searches, health apps for monitoring, and e-mails to communicate about health issues. The research team found a range of benefits (more informed patients) and downsides (overwhelming information) to using new technologies, and the need for support, guidance and education for both patients and providers.
ACE is proud to report that the 2014 Canadian Institutes of Health Research (CIHR) Partnership Award has been awarded to Arthritis Research Canada and its Scientific Director, Dr. John Esdaile, in collaboration with Arthritis Consumer Experts (ACE) and Shoppers Drug Mart/Pharmaprix, for an innovative screening program to help Canadians better prevent and manage arthritis. Through the Shoppers Drug Mart Arthritis Screening Program, these partners have shown how researchers, patients and the private sector can work together to provide health solutions to Canadians. The three partners developed the arthritis screening program following research undertaken at Arthritis Research Canada that showed an early intervention right at the pharmacy counter could accurately diagnose osteoarthritis of the knee and help the person seek appropriate medical attention and best utilize over-the-counter treatments.
 “On behalf of CIHR, I congratulate Arthritis Research Canada and its partners for their innovative efforts to make arthritis screening and management more accessible. We are pleased to have funded research that contributed to the development of this important program. This partnership clearly demonstrates how multiple organizations and individuals can come together for the benefit of Canadians,” said Michel Perron Vice-President, External Affairs and Business Development, CIHR.
“On behalf of CIHR, I congratulate Arthritis Research Canada and its partners for their innovative efforts to make arthritis screening and management more accessible. We are pleased to have funded research that contributed to the development of this important program. This partnership clearly demonstrates how multiple organizations and individuals can come together for the benefit of Canadians,” said Michel Perron Vice-President, External Affairs and Business Development, CIHR.
As part of the program, pharmacists at more than 1,200 Shoppers Drug Mart stores across Canada have provided arthritis screening and information to Canadians. To help detect the disease at an early stage, the program includes a self-administered joint exam and questionnaire. It also enables Canadians with arthritis to work with a pharmacist to monitor their symptoms and medication over time to prevent the disease from worsening. The Shoppers Drug Mart Arthritis Screening Program is the first and only program in Canada designed especially for women afflicted with arthritis. The disease affects two out of three or 2.8 million Canadian women.
Commenting on the award, Cheryl Koehn, Founder and President of ACE, said: “Canada’s more than 4.6 million arthritis consumers, who ACE helps represent, have benefited greatly from this collaboration between ACE, our scientific partner, Arthritis Research Canada, and Shoppers Drug Mart/Pharmaprix. Together, we have created a best practice in Canada for arthritis screening, prevention and management at convenient pharmacy locations on main streets across Canada, right where Canadians with arthritis live and work. ACE is proud to have played a co-leading role to enable Shoppers’ pharmacists to share valuable arthritis information and detect or confirm arthritis with patients through innovative consumer education programs right at the pharmacy counter.”
 ACE co-defended, along with researchers from Arthris Research Canada, a poster presentation at the Canadian Rheumatology Association Annual Scientific Meeting. The presentation involved a survey of Canadians’ priorities and views about using digital media in arthritis prevention and treatment.
ACE co-defended, along with researchers from Arthris Research Canada, a poster presentation at the Canadian Rheumatology Association Annual Scientific Meeting. The presentation involved a survey of Canadians’ priorities and views about using digital media in arthritis prevention and treatment.
The study surveyed Canadians to assess their views and priorities in using digital media in arthritis management in both English and French, asking what people with musculoskeletal (or bones, muscles and joints) problems and their caretakers thought about the challenges with arthritis prevention and treatment. The study also asked them about what they thought the role of digital media is for managing RA. here are some of the findings:
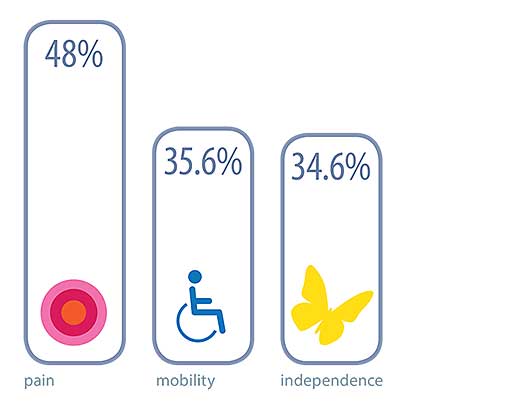
Challenges
Respondents identified pain (48%), loss of mobility (35.6%), and loss of functional independence (34.6%) as main challenges faced by people with arthritis.
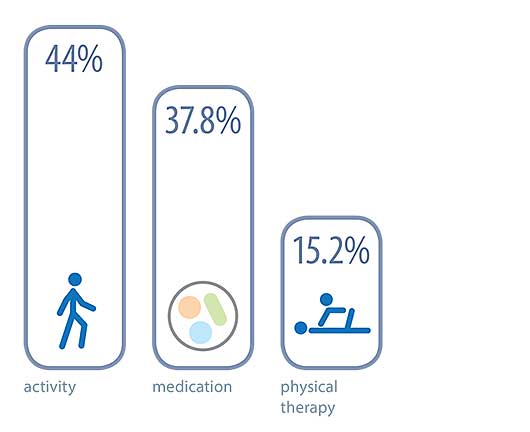
Treatment Strategies
Physical activity (44%), medication (37.8%) and physical therapy (15.2%) were the most mentioned treatment strategies
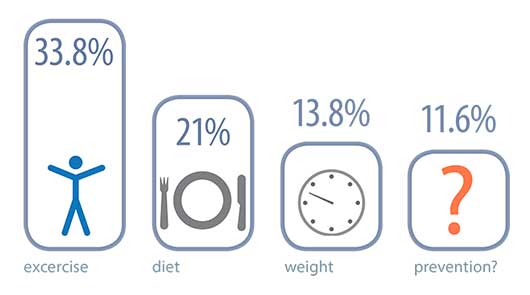
Prevention
Exercise (33.8%), diet (21%) and healthy body weight (13.8%) were the most mentioned prevention strategies, 11.6% did not know how it could be prevented
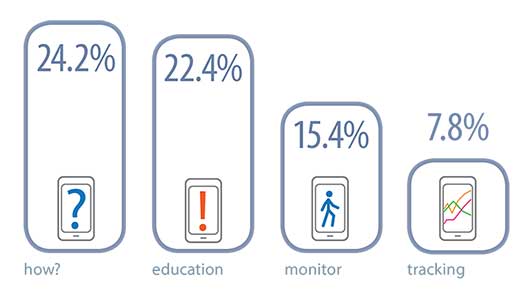
Digital Media
24.2% did not know how it could be used, 22.4% felt that digital media could provide education material, monitor exercise (15.4%), and track symptoms (7.8%).
Listening to you
We hope you find this information of use. Please tell us what you think by writing to us or emailing us at info@jointhealth.org. Through your ongoing and active participation, ACE can make its work more relevant to all Canadians living with arthritis.
Update your email or postal address
Please let us know of any changes by contacting ACE at info@jointhealth.org. This will ensure that you continue to receive your free email or print copy of JointHealth™ monthly.
Arthritis Consumer Experts (ACE)
Who We Are
Arthritis Consumer Experts (ACE) provides research-based education, advocacy training, advocacy leadership and information to Canadians with arthritis. We help empower people living with all forms of arthritis to take control of their disease and to take action in healthcare and research decision making. ACE activities are guided by its members and led by people with arthritis, leading medical professionals and the ACE Advisory Board. To learn more about ACE, visit: www.jointhealth.org
Acknowledgements
Over the past 12 months, ACE received unrestricted grants-in-aid from: AbbVie Corporation, Amgen Canada, Arthritis Research Canada, BIOTECanada, Bristol-Myers Squibb Canada, Canadian Institutes of Health Research, the Canadian Rheumatology Research Consortium, Celgene Inc., GlaxoSmithKline, Hoffman-La Roche Canada Ltd., Janssen Inc., Pfizer Canada, Purdue Pharma L.P., Sanofi Canada, St. Paul’s Hospital (Vancouver) and the University of British Columbia. ACE also receives unsolicited donations from its community members (people with arthritis) across Canada. ACE thanks these private and public organizations and individuals.
ACE thanks these private and public organizations and individuals.
Disclaimer
The material contained on this website is provided for general information only. This website should not be relied on to suggest a course of treatment for a particular individual or as a substitute for consultation with qualified health professionals who are familiar with your individual medical needs. Should you have any healthcare related questions, you should contact your physician. You should never disregard medical advice or delay in seeking it because of something you have read on this or any website.
This site may provide links to other Internet sites only for the convenience of World Wide Web users. ACE is not responsible for the availability or content of these external sites, nor does ACE endorse, warrant or guarantee the products, services or information described or offered at these other Internet sites.
Although the information presented on this website is believed to be accurate at the time it is posted, this website could include inaccuracies, typographical errors or out-of-date information. This website may be changed at any time without prior notice.
Turn back the clock 15 years ago when Arthritis Consumer Experts was founded, when new research began to suggest that osteoarthritis started attacking joints long before middle age, even before a person experienced symptoms of pain and inflammation. A paradigm shift in arthritis understanding was occurring and would deeply impact patients and their families, government and employers. Back in 2000, the world for people with arthritis was on the verge of dramatic transformation based on this new research and with the introduction of biologic therapy for inflammatory types of arthritis, like rheumatoid arthritis, a driver of indirect healthcare costs and a leading cause of work disability in Canada. Fast-forward to today and the scene looks much different. With well-trained Canadian researchers continuing to work and lead in collaboration with their counterparts around the world, the words “prevention” and “remission” are heard in rheumatology offices across the country. Pain is being reduced, quality of life is improving, and work disability is dropping in people with arthritis who would have done much worse had the knowledge from research not been utilized in their model of care.
In this JointHealth™ monthly, we look at research stories that demonstrate the value of collaboration between those who conduct research and those who use its results – consumers like us, people living with arthritis.
This collection of stories highlights the significant impacts arthritis research can achieve. Although each is different, as a group, they exemplify the commitment of Canadian researchers to improving the health of Canadians living with arthritis.
“Treat-to-target” and “window of opportunity”: what do they mean for you?
At conferences hosted by the American College of Rheumatology or the Canadian Rheumatology Association, one hears and reads research findings about “treat-to-target” and “window of opportunity”. What do these findings mean for people living with all types of arthritis?
Opening a “window of opportunity”
With no arthritis cure available, doctors in the past did little more than manage a patient’s pain, explains Dr. Kam Shojania, a rheumatologist and Clinical Professor and Chief, Division of Rheumatology, The University of British Columbia.
“Now, we see that the best therapy is early,” he says, adding that if doctors prescribe disease-modifying drugs for inflammatory forms of arthritis within the early weeks or first six months of disease onset, the chance of putting them into long-term remission go up significantly.
“If you miss that window of opportunity, it’s very sad. You can still treat it, but you are not going to put them in remission. And any damage that has already occurred prior to proper treatment can never be reversed.”
The “window of opportunity” for early treatment of rheumatoid arthritis (RA) within six weeks after positive diagnosis is critical to help avoid or lessen joint damage, produce disease remission and preserve joint integrity since it is documented that joint damage begins within this time frame. For example, if a person with newly diagnosed RA is started on triple DMARD therapy, the need for stronger, more expensive medications will be delayed or not needed all together. As well, biologic response modifiers have exhibited significant clinical benefit in the treatment of early RA (methotrexate naïve patients) and also when used together with methotrexate.
| Research on the “window of opportunity” demonstrates the importance to arthritis patients and the healthcare system for early, aggressive treatment “cocktails” as early as possible after disease onset, as practiced with cancer, HIV and other autoimmune disease states. |
The "treat-to-target" concept
Another treatment paradigm for arthritis involves physicians adopting an approach that all RA should be put into remission (remission as the treatment target), with patients nearly, or completely, free of inflammation, pain and other hallmark symptoms. Central to this treatment philosophy is aggressively initiating and swapping medications every two or three months until the therapy combination brings the disease under maximal control.
This concept is called “treat to target” and historically has been used to help with chronic medical conditions like diabetes, high blood pressure, and high cholesterol. The majority of rheumatologists in Canada, the United States and Europe are now taking this approach with their RA and other inflammatory arthritis patients.
Previously, rheumatologists took a more cautious approach to improve symptoms in their patients, which led to smaller improvements of overall health over a longer period of time, measured by percentages (20% or 50%, for example). Today, they work closely with their patients and set a decisive treatment goal – to achieve 100% improvement. Following the “treat-to-target” concept, complete disease control is the focus and means that if successful, patients get their lives back, avoid the permanent joint damage and many of the other negative consequences that RA can cause over time.
The latest research is focused on developing “prediction tools” for the purpose of matching the right quantity and level of care to the right person. This requires following people with newly diagnosed onset RA closely. Central to “treat to target” is rheumatologist and patient assessing all treatment options available, considering which treatment, alone or in combination, is best and setting improvement goals, measuring progress towards them, and then adjusting or continuing with the treatment until complete remission is achieved if at all possible.
Measurements for gauging success can include:
- A patient’s self-assessment of how they feel (like the “HAQ”);
- The doctor’s assessment of the patient’s symptoms, using standardized examination techniques and patient questionnaires;
- Laboratory tests, like measures of inflammatory proteins in the blood that show to what extent RA is being affected by treatment.
Canada has a strong track record as an international leader in arthritis research. At the recent American College of Rheumatology Annual Meeting (November 2014), attended by leading researchers from around the world, studies led by Canadians were plentiful. Here are some of the notable findings presented:
Tools to help arthritis patients self monitor their disease
Erin Carruthers, a Research Assistant at Arthritis Research Canada, led a presentation on “Using patient reported outcome measures to classify disease activity states in rheumatoid arthritis: A Comparison of Patient Activity Score (PAS) and Routine Assessment of Patient Index Data (RAPID)”.
Helping people with rheumatoid arthritis monitor their own disease activity enhances active involvement of people in their care and may help the “treat to target” strategy by alerting patients when targets are not met, indicating a need to see their physician and re-evaluate treatment. The study compared patient reported outcomes to evaluate disease activity by measuring their agreement with disease activity states evaluated by their rheumatologist at the time of a follow-up visit. The results suggest that patients can self-monitor their disease activity using the self-reported questionnaires. One questionnaire, PASII, showed the best agreement with rheumatologist assessments.
Medications in pregnancy for lupus patients
Dr. Mary De Vera, Assistant Professor at UBC’s Faculty of Pharmaceutical Sciences, and her team reported on their study on “Patterns of medication use before, during, and after pregnancy among women with systemic lupus erythematosus: A population-based study”.
Dr. De Vera’s team assessed the use of medications in pregnant women with lupus in British Columbia. Most pregnancy trimesters in the study were exposed to hydroxychloroquine and/or chloroquine (41 to 45% of exposed pregnancy trimesters). The research observed an increase in glucocorticosteroid (like prednisone) exposures during pregnancy, as well as post-delivery. Findings emphasize the importance of counseling women regarding childbearing decisions as well as the need for evaluation of the risk-benefit profiles of medications in pregnancy.
Arthritis and a First Nations population
Dr. Cheryl Barnabe, a leading researcher at the University of Calgary, has lead a team of researchers on a study on the prevalence of inflammatory arthritis diseases in the First Nations population of Alberta.
Rheumatoid arthritis, ankylosing spondylitis and reactive arthritis were estimated as being twice as frequent in the First Nations population. This research study found, in contrast, psoriatic arthritis was slightly less frequent in First Nations. Crystal arthritis like gout surpassed rheumatoid arthritis as the most frequent type of inflammatory arthritis in the non-First Nations population, with a frequency three times that of the First Nations cohort.
Patients and healthcare professionals using technology
Dr. Anne Townsend, Research Associate, Department of Occupational Science and Occupational Therapy at the University of British Columbia, shared findings from her team’s research on “Aligning ethics with digital health technologies and shared decision-making: Interview accounts of patients and clinicians”.
Patients with different types of arthritis and at least one other health condition, and healthcare providers were interviewed to find out how they used different types of new health technologies such as the Internet for online information searches, health apps for monitoring, and e-mails to communicate about health issues. The research team found a range of benefits (more informed patients) and downsides (overwhelming information) to using new technologies, and the need for support, guidance and education for both patients and providers.
ACE is proud to report that the 2014 Canadian Institutes of Health Research (CIHR) Partnership Award has been awarded to Arthritis Research Canada and its Scientific Director, Dr. John Esdaile, in collaboration with Arthritis Consumer Experts (ACE) and Shoppers Drug Mart/Pharmaprix, for an innovative screening program to help Canadians better prevent and manage arthritis. Through the Shoppers Drug Mart Arthritis Screening Program, these partners have shown how researchers, patients and the private sector can work together to provide health solutions to Canadians. The three partners developed the arthritis screening program following research undertaken at Arthritis Research Canada that showed an early intervention right at the pharmacy counter could accurately diagnose osteoarthritis of the knee and help the person seek appropriate medical attention and best utilize over-the-counter treatments.
“On behalf of CIHR, I congratulate Arthritis Research Canada and its partners for their innovative efforts to make arthritis screening and management more accessible. We are pleased to have funded research that contributed to the development of this important program. This partnership clearly demonstrates how multiple organizations and individuals can come together for the benefit of Canadians,” said Michel Perron Vice-President, External Affairs and Business Development, CIHR.As part of the program, pharmacists at more than 1,200 Shoppers Drug Mart stores across Canada have provided arthritis screening and information to Canadians. To help detect the disease at an early stage, the program includes a self-administered joint exam and questionnaire. It also enables Canadians with arthritis to work with a pharmacist to monitor their symptoms and medication over time to prevent the disease from worsening. The Shoppers Drug Mart Arthritis Screening Program is the first and only program in Canada designed especially for women afflicted with arthritis. The disease affects two out of three or 2.8 million Canadian women.
Commenting on the award, Cheryl Koehn, Founder and President of ACE, said: “Canada’s more than 4.6 million arthritis consumers, who ACE helps represent, have benefited greatly from this collaboration between ACE, our scientific partner, Arthritis Research Canada, and Shoppers Drug Mart/Pharmaprix. Together, we have created a best practice in Canada for arthritis screening, prevention and management at convenient pharmacy locations on main streets across Canada, right where Canadians with arthritis live and work. ACE is proud to have played a co-leading role to enable Shoppers’ pharmacists to share valuable arthritis information and detect or confirm arthritis with patients through innovative consumer education programs right at the pharmacy counter.”
ACE co-defended, along with researchers from Arthris Research Canada, a poster presentation at the Canadian Rheumatology Association Annual Scientific Meeting. The presentation involved a survey of Canadians’ priorities and views about using digital media in arthritis prevention and treatment.The study surveyed Canadians to assess their views and priorities in using digital media in arthritis management in both English and French, asking what people with musculoskeletal (or bones, muscles and joints) problems and their caretakers thought about the challenges with arthritis prevention and treatment. The study also asked them about what they thought the role of digital media is for managing RA. here are some of the findings:
Challenges
Respondents identified pain (48%), loss of mobility (35.6%), and loss of functional independence (34.6%) as main challenges faced by people with arthritis.
Treatment Strategies
Physical activity (44%), medication (37.8%) and physical therapy (15.2%) were the most mentioned treatment strategies
Prevention
Exercise (33.8%), diet (21%) and healthy body weight (13.8%) were the most mentioned prevention strategies, 11.6% did not know how it could be prevented
Digital Media
24.2% did not know how it could be used, 22.4% felt that digital media could provide education material, monitor exercise (15.4%), and track symptoms (7.8%).
| Overall, this survey uncovered gaps in the awareness of arthritis prevention and treatment, and the perceived role of digital media, presenting opportunities for future work and collaboration between ACE and researchers to advance knowledge translation in this important area. |
Listening to you
We hope you find this information of use. Please tell us what you think by writing to us or emailing us at info@jointhealth.org. Through your ongoing and active participation, ACE can make its work more relevant to all Canadians living with arthritis.
Update your email or postal address
Please let us know of any changes by contacting ACE at info@jointhealth.org. This will ensure that you continue to receive your free email or print copy of JointHealth™ monthly.
Arthritis Consumer Experts (ACE)
Who We Are
Arthritis Consumer Experts (ACE) provides research-based education, advocacy training, advocacy leadership and information to Canadians with arthritis. We help empower people living with all forms of arthritis to take control of their disease and to take action in healthcare and research decision making. ACE activities are guided by its members and led by people with arthritis, leading medical professionals and the ACE Advisory Board. To learn more about ACE, visit: www.jointhealth.org
Acknowledgements
Over the past 12 months, ACE received unrestricted grants-in-aid from: AbbVie Corporation, Amgen Canada, Arthritis Research Canada, BIOTECanada, Bristol-Myers Squibb Canada, Canadian Institutes of Health Research, the Canadian Rheumatology Research Consortium, Celgene Inc., GlaxoSmithKline, Hoffman-La Roche Canada Ltd., Janssen Inc., Pfizer Canada, Purdue Pharma L.P., Sanofi Canada, St. Paul’s Hospital (Vancouver) and the University of British Columbia. ACE also receives unsolicited donations from its community members (people with arthritis) across Canada. ACE thanks these private and public organizations and individuals.
ACE thanks these private and public organizations and individuals.
Disclaimer
The material contained on this website is provided for general information only. This website should not be relied on to suggest a course of treatment for a particular individual or as a substitute for consultation with qualified health professionals who are familiar with your individual medical needs. Should you have any healthcare related questions, you should contact your physician. You should never disregard medical advice or delay in seeking it because of something you have read on this or any website.
This site may provide links to other Internet sites only for the convenience of World Wide Web users. ACE is not responsible for the availability or content of these external sites, nor does ACE endorse, warrant or guarantee the products, services or information described or offered at these other Internet sites.
Although the information presented on this website is believed to be accurate at the time it is posted, this website could include inaccuracies, typographical errors or out-of-date information. This website may be changed at any time without prior notice.
