In this issue
- Background
- Who were the Survey respondents?
- Finding, processing and using health informationn
- Using information in decision making
- Implications for arthritis care
JointHealth™ insight Published November 2023


Listening to you
We hope you find this information of use. Please tell us what you think by writing to us or emailing us at feedback@jointhealth.org. Through your ongoing and active participation, ACE can make its work more relevant to all Canadians living with arthritis.
Update your email or postal address
Please let us know of any changes by contacting ACE at feedback@jointhealth.org. This will ensure that you continue to receive your free email or print copy of JointHealth™ insight.
Arthritis Consumer Experts (ACE)
Who We Are
Arthritis Consumer Experts (ACE) and its team members acknowledge that they gather and work on the traditional, ancestral and unceded territory of the Coast Salish peoples -ʷməθkʷəy̓əm (Musqueam), Sḵwx̱wú7mesh (Squamish), and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) Nations.
Arthritis Consumer Experts (ACE) operates as a non-profit and provides free research based education and information to Canadians with arthritis. We help (em)power people living with all forms of arthritis to take control of their disease and to take action in healthcare and research decision making. ACE activities are guided by its members and led by people with arthritis, scientific and medical experts on the ACE Advisory Board. To learn more about ACE, visit www.jointhealth.org
Disclosures
Over the past 12 months, ACE received grants-in-aid from: Amgen Canada, Arthritis Research Canada, Biosimilars Canada, Canadian Biosimilars Forum, Canadian Rheumatology Association, Eli Lilly Canada, JAMP Pharma, Novartis Canada, Organon Canada, Pfizer Canada, Sandoz Canada, Teva Canada, UCB Canada, the University of British Columbia, and the University of Toronto.
ACE also received unsolicited donations from its community members (people with arthritis) across Canada.
ACE thanks funders for their support to help the nearly 6 million Canadians living with osteoarthritis, rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and the many other forms of the disease.
Disclaimer
The material contained on this website is provided for general information only. This website should not be relied on to suggest a course of treatment for a particular individual or as a substitute for consultation with qualified health professionals who are familiar with your individual medical needs. Should you have any healthcare related questions, you should contact your physician. You should never disregard medical advice or delay in seeking it because of something you have read on this or any website.
This site may provide links to other Internet sites only for the convenience of World Wide Web users. ACE is not responsible for the availability or content of these external sites, nor does ACE endorse, warrant or guarantee the products, services or information described or offered at these other Internet sites.
Although the information presented on this website is believed to be accurate at the time it is posted, this website could include inaccuracies, typographical errors or out-of-date information. This website may be changed at any time without prior notice.
Arthritis Consumer Experts (ACE) is committed to taking action to address inequities in arthritis care and we recognize it takes the whole community to make positive change. From June 1 to 25, 2023, ACE conducted a 40-question national online Survey in English and French to understand health literacy levels of people living with arthritis. People who responded answered questions about their socioeconomic status, ability to understand and use health information, interactions with health care providers, ability to use information in decision making, self-care and how they increase health knowledge.
This JointHealth™ insight is Part 2 of the ACE National Survey on Arthritis and Health Literacy findings analysis. We take a deeper look at the responses from Black, Indigenous, and people of colour (BIPOC) versus white respondents.
 Background
Background
What is health literacy?
The Canadian Public Health Association Expert Panel on Health Literacy defines health literacy as “the ability to access, understand, evaluate and communicate information as a way to promote, maintain and improve health in a variety of settings across the life course.” The results of limited health literacy are barriers to accessing health services, development or worsening of chronic illness and preventable disease, and ineffective use of health services.1
Health information is constantly changing and being updated and delivered in multiple ways – as online resources, information pamphlets, through videos, infographics, and podcasts. In an Arthritis At Home interview with Dr. Fiona Rawle, Associate Dean, Pedagogical Development and Scholarship, Dr. Rawle discusses ways to recognize fake science and health information and tips on communicating science to patients.
 Who were the Survey respondents?
Who were the Survey respondents?
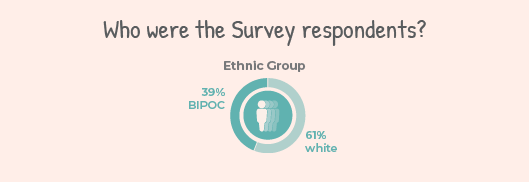
A total of 1,148 people responded to the Survey. These people will be referred to in this writing as “respondents.” Out of the total respondents, 449 (39%) were BIPOC and 699 (61%) were white. We received 48 responses from respondents who identified as Black, 280 from those who identified as Indigenous, and 121 from those who identified as a person of colour. For more demographic information including education, income, and type of arthritis, please refer to the Appendix at the end of this newsletter.
 What did we find?
What did we find?
Understanding and using health information
Navigating the world of health information can be challenging. Information can come from online content and mainstream media sources to opinions and advice from family and friends. It's important to understand health information and apply it to communicate effectively with health care providers and make informed decisions.
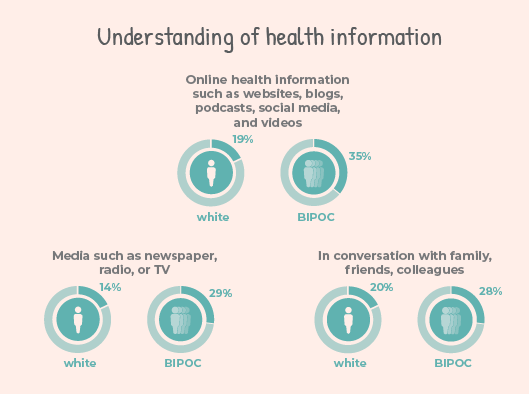
Our Survey findings show that while BIPOC and white respondents have similar levels of understanding of health information, BIPOC respondents reported higher levels of understanding when compared to white respondents. This was particularly true for information found online, in the media, and in conversations with family and friends (BIPOC vs white):
 Talking with health care providers
Talking with health care providers
Health information should be delivered in a way that is easy to understand to ensure people with arthritis feel included, safe, heard, and understood in conversations about their health. To understand the level of interaction between people living with arthritis and their health care providers, Survey respondents were asked how often their health care providers:
 Using information to make better health decisions
Using information to make better health decisions
Using health information to make choices is very important. It helps people understand their health challenges, choose the best treatments, participate in physical activities that are most suitable to them, and make healthy food choices. ACE asked people to rate their ability to use information to make decisions on a scale from 1 (not confident) to 5 (very confident).
BIPOC resondents, when compared to white respondents, reported lower levels of understanding of the purpose of each medication (32% vs 62%), how much medication to take (38% vs 70%) and experience greater challenges taking medication the way it was prescribed (20% vs 6%). Similar lower levels of understanding were observed for understanding the purpose of physical activity (28% vs 60%), knowing how, where, and when to participate in physical activity (24% vs 45%); as well as the purpose of a healthy diet (32% vs 57%) and reading food labels (20% vs 31%). There were no differences between BIPOC and white respondents in their confidence to participate in physical activity or knowledge of what foods to avoid.
Taking care of yourself
Taking care of yourself, or “self-care,” is an important part of managing arthritis. This can include seeking help from others, using reliable online resources or going to educational workshops and webinars. Doing these things help people with arthritis learn more about how to manage and take control of their health.
BIPOC respondents reported attending workshops or webinars more often than white respondents (42% vs 19%), going to support group meetings (48% vs 13%), and following self-help guides online (56% vs 48%). However, BIPOC respondents were much less willing to ask others for help than white respondents (20% vs 37%). This may suggest that they may be facing a cultural barrier when looking for help. According to a 2017 review by the Wellesley Institute, receiving care in a language you don’t understand often leads to poorer health outcomes. These include a higher risk of receiving inappropriate medical testing, an increased risk of hospitalization and adverse medication reactions, and decreased patient satisfaction2.
Learning more about health and arthritis
Increasing health knowledge and skills supports people with arthritis to better learn about new medication and non- medication treatments, understand research, and deal with changes in health. ACE asked people how they want to improve their health literacy and most reported they preferred learning from a health care provider. However, there were some discrepancies between BIPOC and white respondents.
BIPOC respondents (more often than white respondents) selected:
“1 on 1 counselling” (35% vs 30%)
“Online community or support groups” (42% vs 19%)
“From other patients” (19% vs 12%)
White respondents (more often than BIPOC) selected:
“I am confident in my current health knowledge and skills” (25% vs 2%)
How can ACE’s Survey results inform arthritis care in Canada?
The Arthritis Consumer Experts Health Literacy Survey Part 2 provides valuable insights into the challenges and needs of BIPOC individuals living with arthritis. It shows us how health literacy is very important to the self-care of arthritis and the various experiences using health information and learning preferences among people living with arthritis in the BIPOC community.
Our findings show that BIPOC and white respondents have similar levels of understanding of health information. However, BIPOC respondents reported facing disproportionate challenges when talking with health care providers and feeling less listened to during interactions. BIPOC respondents also reported facing barriers when navigating health care services and challenges with medications, physical activity, diet, and self-care due to the inequitable policies and structures that are in place.
Interestingly, our findings revealed that BIPOC respondents (when compared to white), have unique preferences when it comes to gaining knowledge and were much less willing to ask others for help. This may suggest BIPOC respondents face barriers when looking for help and highlights the need for health care providers to provide appropriate and sensitive care to those with diverse cultural and linguistic backgrounds. The creation of targeted resources and services that meet the needs of specific populations is a priority. These resources must be made available to patients, care givers, and health care providers at all points of a patient’s journey.
Read our Part 1 analysis of the ACE National Survey on Arthritis and Health Literacy to learn what people living with arthritis, health care providers, and policymakers can do to support and improve health literacy.

Resources on health literacy and services for BIPOC populations can be found here:
References

Appendix
Table 1: Sociodemographic information
*Percentages do not add to 100% due to missing values and/or round off.
This JointHealth™ insight is Part 2 of the ACE National Survey on Arthritis and Health Literacy findings analysis. We take a deeper look at the responses from Black, Indigenous, and people of colour (BIPOC) versus white respondents.
What is health literacy?
The Canadian Public Health Association Expert Panel on Health Literacy defines health literacy as “the ability to access, understand, evaluate and communicate information as a way to promote, maintain and improve health in a variety of settings across the life course.” The results of limited health literacy are barriers to accessing health services, development or worsening of chronic illness and preventable disease, and ineffective use of health services.1
Health information is constantly changing and being updated and delivered in multiple ways – as online resources, information pamphlets, through videos, infographics, and podcasts. In an Arthritis At Home interview with Dr. Fiona Rawle, Associate Dean, Pedagogical Development and Scholarship, Dr. Rawle discusses ways to recognize fake science and health information and tips on communicating science to patients.
Who were the Survey respondents?A total of 1,148 people responded to the Survey. These people will be referred to in this writing as “respondents.” Out of the total respondents, 449 (39%) were BIPOC and 699 (61%) were white. We received 48 responses from respondents who identified as Black, 280 from those who identified as Indigenous, and 121 from those who identified as a person of colour. For more demographic information including education, income, and type of arthritis, please refer to the Appendix at the end of this newsletter.
What did we find?Understanding and using health information
Navigating the world of health information can be challenging. Information can come from online content and mainstream media sources to opinions and advice from family and friends. It's important to understand health information and apply it to communicate effectively with health care providers and make informed decisions.
Our Survey findings show that while BIPOC and white respondents have similar levels of understanding of health information, BIPOC respondents reported higher levels of understanding when compared to white respondents. This was particularly true for information found online, in the media, and in conversations with family and friends (BIPOC vs white):
- Online health information such as websites, blogs, podcasts, social media, and videos – BIPOC at 35% vs white at 19%
- Media such as newspaper, radio, or TV – BIPOC at 29% vs white at 14%
- In conversation with family, friends, colleagues – BIPOC at 28% vs white at 20%
Talking with health care providersHealth information should be delivered in a way that is easy to understand to ensure people with arthritis feel included, safe, heard, and understood in conversations about their health. To understand the level of interaction between people living with arthritis and their health care providers, Survey respondents were asked how often their health care providers:
- explained health issues in a way that is easy to understand
- used medical terms or words that Survey respondent did not understand
- used visuals including pictures, drawings, models, or videos to demonstrate how to take the medication, use an assistive device or follow a technique
- listened carefully to Survey respondent
- encouraged Survey respondent to ask questions
Using information to make better health decisionsUsing health information to make choices is very important. It helps people understand their health challenges, choose the best treatments, participate in physical activities that are most suitable to them, and make healthy food choices. ACE asked people to rate their ability to use information to make decisions on a scale from 1 (not confident) to 5 (very confident).
BIPOC resondents, when compared to white respondents, reported lower levels of understanding of the purpose of each medication (32% vs 62%), how much medication to take (38% vs 70%) and experience greater challenges taking medication the way it was prescribed (20% vs 6%). Similar lower levels of understanding were observed for understanding the purpose of physical activity (28% vs 60%), knowing how, where, and when to participate in physical activity (24% vs 45%); as well as the purpose of a healthy diet (32% vs 57%) and reading food labels (20% vs 31%). There were no differences between BIPOC and white respondents in their confidence to participate in physical activity or knowledge of what foods to avoid.
Taking care of yourself
Taking care of yourself, or “self-care,” is an important part of managing arthritis. This can include seeking help from others, using reliable online resources or going to educational workshops and webinars. Doing these things help people with arthritis learn more about how to manage and take control of their health.
BIPOC respondents reported attending workshops or webinars more often than white respondents (42% vs 19%), going to support group meetings (48% vs 13%), and following self-help guides online (56% vs 48%). However, BIPOC respondents were much less willing to ask others for help than white respondents (20% vs 37%). This may suggest that they may be facing a cultural barrier when looking for help. According to a 2017 review by the Wellesley Institute, receiving care in a language you don’t understand often leads to poorer health outcomes. These include a higher risk of receiving inappropriate medical testing, an increased risk of hospitalization and adverse medication reactions, and decreased patient satisfaction2.
Learning more about health and arthritis
Increasing health knowledge and skills supports people with arthritis to better learn about new medication and non- medication treatments, understand research, and deal with changes in health. ACE asked people how they want to improve their health literacy and most reported they preferred learning from a health care provider. However, there were some discrepancies between BIPOC and white respondents.
BIPOC respondents (more often than white respondents) selected:
“1 on 1 counselling” (35% vs 30%)
“Online community or support groups” (42% vs 19%)
“From other patients” (19% vs 12%)
White respondents (more often than BIPOC) selected:
“I am confident in my current health knowledge and skills” (25% vs 2%)
How can ACE’s Survey results inform arthritis care in Canada?
The Arthritis Consumer Experts Health Literacy Survey Part 2 provides valuable insights into the challenges and needs of BIPOC individuals living with arthritis. It shows us how health literacy is very important to the self-care of arthritis and the various experiences using health information and learning preferences among people living with arthritis in the BIPOC community.
Our findings show that BIPOC and white respondents have similar levels of understanding of health information. However, BIPOC respondents reported facing disproportionate challenges when talking with health care providers and feeling less listened to during interactions. BIPOC respondents also reported facing barriers when navigating health care services and challenges with medications, physical activity, diet, and self-care due to the inequitable policies and structures that are in place.
Interestingly, our findings revealed that BIPOC respondents (when compared to white), have unique preferences when it comes to gaining knowledge and were much less willing to ask others for help. This may suggest BIPOC respondents face barriers when looking for help and highlights the need for health care providers to provide appropriate and sensitive care to those with diverse cultural and linguistic backgrounds. The creation of targeted resources and services that meet the needs of specific populations is a priority. These resources must be made available to patients, care givers, and health care providers at all points of a patient’s journey.
Read our Part 1 analysis of the ACE National Survey on Arthritis and Health Literacy to learn what people living with arthritis, health care providers, and policymakers can do to support and improve health literacy.
Resources on health literacy and services for BIPOC populations can be found here:
- Public Health Association of BC: An Inter-sectoral Approach for Improving Health Literacy for Canadians, 2012
- Arthritis At Home 164: Communicating science to patients and ways to recognize pseudoscience
- Arrive: Navigating the health care system in Canada
- Multicultural Mental Health Resource Centre
- OPTIKNEE clinical recommendations to guide rehabilitation to improve knee health and prevent osteoarthritis after a traumatic knee injury
- Provincial Health Services Authority: Translation Services
References
- Health Literacy in Canada: A Healthy Understanding – Canadian Council on Learning, 2008
- Laher, N, A Sultana, A Aery, and N Kumar. Access to Language Interpretation Services and Its Impact on Clinical and Patient Outcomes: A Scoping Review. Wellesley Institute. (2018).
Appendix
Table 1: Sociodemographic information
| Progress-Plus Framework | |
| Place of residence* | |
|
Large urban centre (population of 100,000+) Small-medium sized population centre (population of 16,000 to 99,999) Rural or remote community (population of 15,999 or less) Reside on a First Nations, Metis, or Inuit reserve/settlement I prefer not to answer this question |
670 246 184 36 12 |
| Canadian province or territory | |
|
British Columbia Alberta Saskatchewan Manitoba Ontario Quebec Nova Scotia New Brunswick Newfoundland and Labrador Prince Edward Island Northwest Territories Yukon Nunavut I live outside of Canada |
203 143 72 68 410 104 49 25 41 14 7 4 2 6 |
| Language | |
|
English French An Indigenous language Other |
973 113 10 52 |
| Ethnic group | |
|
White Black, Indigenous and Person of Colour TOTAL Black Indigenous Two-spirited Person of Colour |
449 601 48 280 152 121 |
| Gender* | |
|
Woman Man Cisgender Transgender Non-binary I prefer not to answer this question I prefer to describe myself as _______ |
610 493 12 5 8 18 2 |
| Education* | |
|
Less than high school High school or equivalent Some college or university College or university graduate I prefer not to answer this question |
33 211 224 673 7 |
| Socioeconomic status (Annual income)* | |
|
$40,000 or lower $40,001 - $80,000 $80,001 or higher I prefer not to answer this question |
224 429 442 53 |
| Social capital (How far do you have to travel to see a health care provider?) | |
|
0-10 kilometres (0-6 miles) 11-25 kilometres (7-15 miles) 26-50 kilometres (16-31 miles) 51-100 kilometres (32-62 miles) 101-250 kilometres (63-155 miles) 251-500 kilometres (156-311 miles) More than 500 kilometres (more than 311 miles) |
453 354 189 77 45 22 8 |
| Plus (Age) | |
|
before 1910 between 1910-1929 between 1930-1949 between 1950-1969 between 1970-1989 between 1990-2009 2010 to present |
2 7 94 345 386 312 2 |
| Time since diagnosis | |
|
0-1 year 2-5 years 6-10 years 11-15 years More than 15 years I did not receive a diagnosis of arthritis |
173 445 278 105 140 7 |
| Plus (Type of arthritis)* | |
|
Adult-onset Still’s disease Ankylosing spondylitis Fibromyalgia Gout Juvenile idiopathic arthritis Lupus Non-radiographic axial spondyloarthritis (not visible on X-ray) Osteoarthritis Polymyalgia rheumatica Psoriatic arthritis Rheumatoid arthritis Scleroderma Sjögrens syndrome Vasculitis Do not know Other |
57 (5%) 80 (7%) 145 (13%) 180 (17% 112 (10%) 89 (8%) 57 (5%) 398 (45%) 88 (8%) 154 (13%) 386 (34%) 81 (7%) 83 (7%) 61 (5%) 83 (7%) 31 (3%) |
*Percentages do not add to 100% due to missing values and/or round off.
Listening to you
We hope you find this information of use. Please tell us what you think by writing to us or emailing us at feedback@jointhealth.org. Through your ongoing and active participation, ACE can make its work more relevant to all Canadians living with arthritis.
Update your email or postal address
Please let us know of any changes by contacting ACE at feedback@jointhealth.org. This will ensure that you continue to receive your free email or print copy of JointHealth™ insight.
Arthritis Consumer Experts (ACE)
Who We Are
Arthritis Consumer Experts (ACE) and its team members acknowledge that they gather and work on the traditional, ancestral and unceded territory of the Coast Salish peoples -ʷməθkʷəy̓əm (Musqueam), Sḵwx̱wú7mesh (Squamish), and Səl̓ílwətaʔ/Selilwitulh (Tsleil-Waututh) Nations.
Arthritis Consumer Experts (ACE) operates as a non-profit and provides free research based education and information to Canadians with arthritis. We help (em)power people living with all forms of arthritis to take control of their disease and to take action in healthcare and research decision making. ACE activities are guided by its members and led by people with arthritis, scientific and medical experts on the ACE Advisory Board. To learn more about ACE, visit www.jointhealth.org
Disclosures
Over the past 12 months, ACE received grants-in-aid from: Amgen Canada, Arthritis Research Canada, Biosimilars Canada, Canadian Biosimilars Forum, Canadian Rheumatology Association, Eli Lilly Canada, JAMP Pharma, Novartis Canada, Organon Canada, Pfizer Canada, Sandoz Canada, Teva Canada, UCB Canada, the University of British Columbia, and the University of Toronto.
ACE also received unsolicited donations from its community members (people with arthritis) across Canada.
ACE thanks funders for their support to help the nearly 6 million Canadians living with osteoarthritis, rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and the many other forms of the disease.
Disclaimer
The material contained on this website is provided for general information only. This website should not be relied on to suggest a course of treatment for a particular individual or as a substitute for consultation with qualified health professionals who are familiar with your individual medical needs. Should you have any healthcare related questions, you should contact your physician. You should never disregard medical advice or delay in seeking it because of something you have read on this or any website.
This site may provide links to other Internet sites only for the convenience of World Wide Web users. ACE is not responsible for the availability or content of these external sites, nor does ACE endorse, warrant or guarantee the products, services or information described or offered at these other Internet sites.
Although the information presented on this website is believed to be accurate at the time it is posted, this website could include inaccuracies, typographical errors or out-of-date information. This website may be changed at any time without prior notice.

